As of mid-2026, the scientific understanding of Long COVID (Post-Acute Sequelae of SARS-CoV-2, or PASC) has shifted from describing symptoms to identifying specific, actionable biological signatures. We are moving out of the “diagnostic mystery” phase and into a period of targeted therapeutic intervention.
Here is what the latest clinical research reveals about the mechanics of the condition and the current roadmap for recovery.
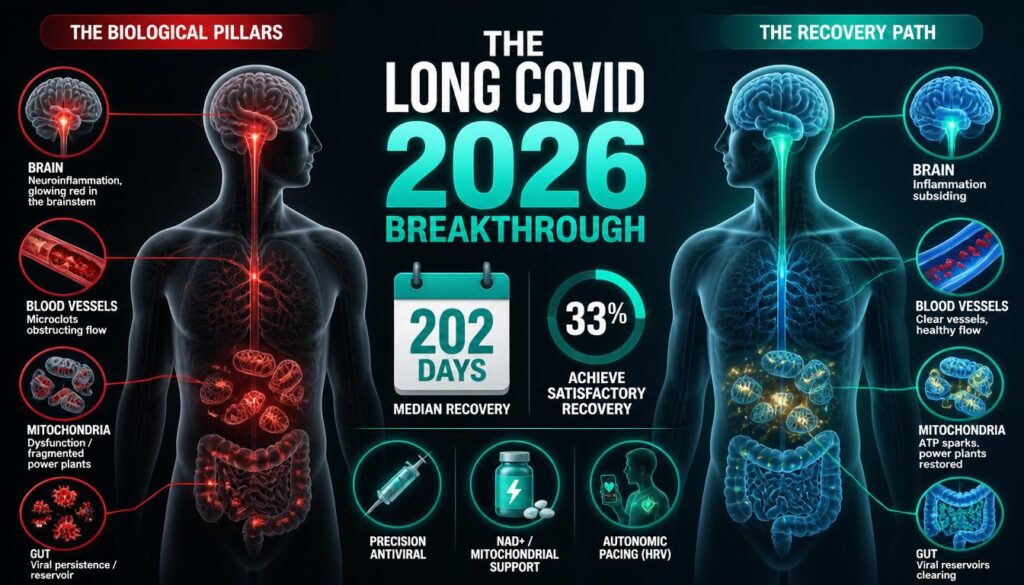
1. The Four Primary Biological Pillars
Clinical trials and longitudinal studies have converged on four primary drivers that explain why patients remain symptomatic long after the initial infection has cleared.
Viral Persistence (The Reservoir Theory)
High-resolution imaging and tissue biopsy studies have confirmed that the SARS-CoV-2 virus, or its protein fragments (specifically spike proteins), can persist in protected “niches”—most notably the gut lining, the brainstem, and the vascular endothelium—triggering chronic immune activation.
Mitochondrial Dysfunction
Researchers have identified a recurring pattern of mitochondrial fragmentation in muscle and immune cells. This explains the hallmark symptom of Post-Exertional Malaise (PEM); the mitochondria are physically unable to ramp up ATP production to meet physical or cognitive demands, leading to a “crash”.
Microclotting and Endothelial Damage
Advanced blood analysis reveals persistent hypercoagulability (micro-clots) that impede capillary blood flow. This restricts oxygen delivery to tissues, explaining the “brain fog” and localized pain reported by patients.
Neuro-inflammation
PET scans have demonstrated ongoing neuro-inflammation in the brainstem and olfactory bulb, suggesting that the virus induces a state of chronic glial cell activation (the brain’s immune system), which disrupts autonomic nervous system regulation.
2. What the Recovery Data Actually Shows
How Long Does Recovery Take?
According to a 4-year prospective cohort analysis of 3,590 individuals with Long COVID, recovery to >75% of pre‑infection health occurred at a median of 202 days (approximately 6.7 months) from symptom onset.
However, recovery is not guaranteed. The same study found that only one‑third (33.4%) of individuals achieved satisfactory recovery.
For those hospitalised with COVID-19, the outlook is even more sobering. The PHOSP-COVID study found that less than 3 in 10 patients reported feeling fully recovered one year after hospital discharge—largely unchanged from 2.5 in 10 at five months.
What Percentage of People Fully Recover?
The data reveals a stark reality: Long COVID recovery rates remain low even years after initial infection. Most patients who have not recovered by five months show little positive change at one year.
Dominant symptoms in Long COVID patients are fatigue (78.7%), breathlessness (68.1%), and brain fog (53.5%).
3. Emerging Therapeutic Approaches
Research in 2026 has focused on moving beyond symptomatic management toward “re‑tuning” the immune and vascular systems.
Precision Antivirals
While early studies showed mixed results, newer, high-dose, long-duration antiviral protocols (specifically targeting the persistence of viral remnants) are showing efficacy in subgroup trials. The goal is to clear the viral reservoirs that keep the immune system in a state of high alert.
Metabolic Resuscitation
Because Long COVID often mimics aspects of Chronic Fatigue Syndrome (ME/CFS), treatments aimed at mitochondrial health are at the forefront. Supplementation strategies focusing on NAD+ precursors and agents that support Coenzyme Q10 synthesis are currently being tested for their ability to restore cellular energy efficiency.
Autonomic Stabilization
Research into the “POTS‑like” symptoms (tachycardia and dizziness) associated with Long COVID has led to increased use of targeted autonomic nervous system modulation. This includes physical pacing combined with specialised pharmacological interventions to stabilise the sympathetic nervous system and reduce the “fight‑or‑flight” loop.
The Japanese Breakthrough: Antibody Biomarkers
Researchers at Okayama University in Japan have made a significant breakthrough, published in April 2026. They found that SARS-CoV-2 antibody patterns may help assess infection history, symptom severity, and cognitive complications in Long COVID.
Key findings:
- N‑antibody levels reflect prior infection severity
- Lower S‑antibody levels are linked to memory problems and poor quality of life
- Women tended to have higher N‑antibody levels than men
- Declining S‑antibody levels may indicate a greater risk of neurological complications
As Professor Fumio Otsuka explained: “Objective biomarkers for LC remain limited, making patient evaluation particularly challenging. Viral antibody titers may help predict the history of COVID-19 infection and may aid in the prognosis of post-COVID-19 symptoms.”
Promising Clinical Trials in 2026
The HPC cord blood therapy (RegeneCyte) is particularly noteworthy: 85% of patients treated reported complete relief from fatigue, compared with only 20% receiving placebo.
4. The Shift in Recovery Strategy: “Aggressive Pacing”
The most significant change in clinical guidance for 2026 is the abandonment of “graded exercise therapy” (which was often harmful to Long COVID patients) in favour of Aggressive Pacing.
Energy Envelope Management
Recovery now relies on strict adherence to an “energy budget.” Patients are encouraged to track their daily capacity using Heart Rate Variability (HRV) monitors. If the patient exceeds their baseline, the resulting PEM (crash) is now understood not just as tiredness, but as a biological setback that triggers further neuro-inflammation.
Anti-Inflammatory Nutrition
There is a strong consensus on the role of a strictly anti‑inflammatory, gut‑microbiome‑focused diet. Since the gut acts as a primary viral reservoir and source of chronic inflammation, restoring mucosal barrier health is now considered a mandatory step in systemic recovery.
5. Why Recovery Takes Time
Data from 2026 reveals that Long COVID is often a “multi‑hit” injury. It is not just the virus; it is the secondary damage to the vascular system, the nervous system, and the microbiome.
The takeaway for recovery is twofold:
- Stop the cycle: The priority is stopping the immune system from constantly reacting to viral debris or damaged cells.
- Cellular repair: Once the inflammatory trigger is minimised, the body’s innate regenerative capacity must be supported through nutrition, controlled autonomic pacing, and, in some cases, targeted pharmacological support.
Summary for Patients
If you are struggling with Long COVID in 2026, the clinical narrative has shifted from “it’s all in your head” to “you have measurable biological dysfunction.”
- Pacing is treatment: Do not push through fatigue. Pushing through PEM is counter‑productive to long‑term recovery.
- Focus on Autonomic Health: If your heart rate spikes upon standing or you suffer from brain fog, discuss autonomic nervous system stabilisation with your physician.
- Monitor inflammation: Biomarker testing for systemic inflammation (like high‑sensitivity CRP) can help your medical team track your progress more objectively.
Disclaimer: This information is for educational purposes based on current clinical trends as of mid‑2026. Long COVID management should always be conducted under the supervision of a qualified medical specialist or a dedicated post‑COVID multidisciplinary team.