The story centers on a 5-month-old infant named Jibran and his family, who became the public face of a high-stakes financial dispute between the state’s largest academic health system and its largest health insurer.
Fortunately for the families involved, the situation has just been resolved. Here is the factual background of the case, the contract dispute, and the latest updates—plus a deeper look at the rare heart condition that put Jibran in the middle of this controversy.
External Link: Official statement from Blue Cross Blue Shield of Michigan available here.
External Link: Michigan Medicine’s C.S. Mott Children’s Hospital web page .
The Medical Crisis: A “Rarest of Rare” Condition
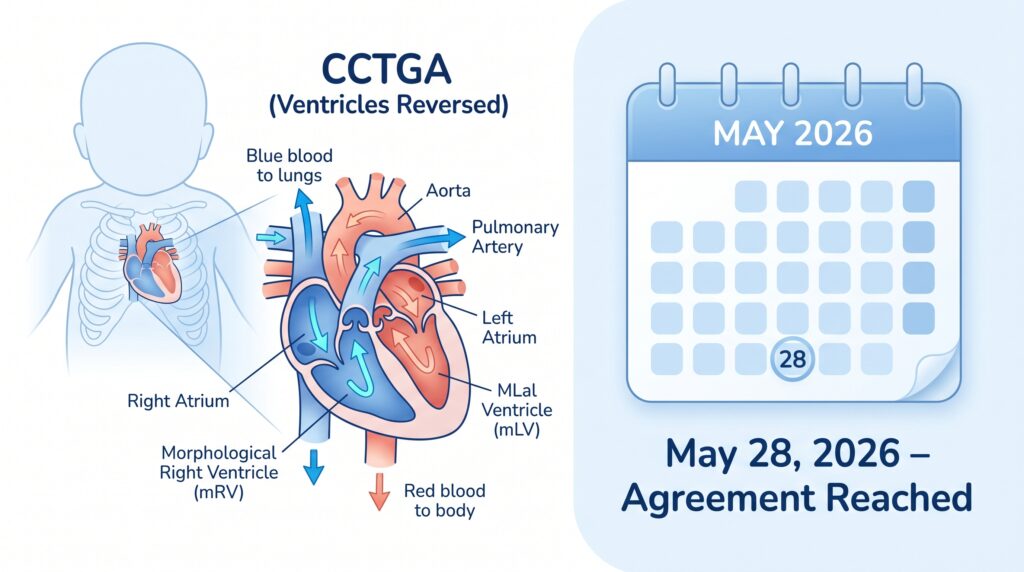
Jibran was born with a severe congenital heart defect known as Congenitally Corrected Transposition of the Great Arteries (CCTGA) .
What Is CCTGA?
To understand CCTGA, imagine the heart as a two‑pump system. Normally, the right ventricle pumps blood to the lungs (short distance, low pressure), and the left ventricle pumps blood to the entire body (long distance, high pressure).
In CCTGA, the ventricles are reversed. The weaker right ventricle is forced to pump blood to the whole body, while the stronger left ventricle pumps to the lungs. Over time, the right ventricle cannot keep up, leading to premature heart failure without intervention.
- Incidence: CCTGA affects less than 0.05% of children born with congenital heart disease – truly a “rarest of rare” condition.
- Associated anomalies: Many children with CCTGA also have other defects, such as ventricular septal defects (VSD) or heart valve abnormalities, which can complicate the clinical picture.
Why Michigan Medicine Is Unique
Due to the extreme complexity of the necessary surgeries—which require stopping the heart and reconstructing its architecture—the family was informed that Michigan Medicine’s C.S. Mott Children’s Hospital is the only facility in the state equipped to perform the procedures. The hospital has a specialized team of pediatric cardiac surgeons and a dedicated congenital heart center that handles some of the most complex cases in the Midwest.
Internal Link: For more on rare disease advocacy and healthcare access, see our guide on Disease Defense .
The Contract Dispute: When Insurance and Hospitals Collide
While Jibran was receiving life‑saving care, a massive financial dispute was playing out behind the scenes between his family’s insurer, Blue Cross Blue Shield of Michigan (BCBSM) , and Michigan Medicine (the University of Michigan’s health system).
The Standoff
- The two entities were struggling to negotiate a new payment contract ahead of a June 30, 2026, expiration date.
- If a deal was not reached, Michigan Medicine would be pushed out‑of‑network for BCBSM members, threatening to displace roughly 300,000 patients statewide.
The Impact on Jibran’s Family
For Jibran’s parents, an out‑of‑network designation would have triggered catastrophic out‑of‑pocket costs. Even with “continuity of care” exceptions, the financial burden of years of specialized cardiac care would be staggering. The family spoke out publicly, arguing that a child’s access to highly specialized, monopolized care should not be used as leverage in a corporate pricing dispute.
The Resolution (May 28, 2026)
The public pressure and looming deadline culminated in a breakthrough. Executives from Blue Cross Blue Shield of Michigan and Michigan Medicine officially announced that they have reached a new, long‑term contract agreement.
While the exact financial terms remain proprietary, the agreement ensures that Michigan Medicine’s hospitals, clinics, and physicians will remain in‑network for Blue Cross members. This resolution effectively ends the threat of a lapse in coverage, ensuring that Jibran and thousands of other patients with complex conditions can continue receiving critical care without facing financial ruin.
Internal Link: Healthcare access is a key component of longevity. Read The Modern Blue Zones Blueprint for more on creating supportive health environments .
Educational Deep Dive: CCTGA – Symptoms, Diagnosis, and Treatment
Symptoms
CCTGA may not cause symptoms at birth. However, as the child grows, the following signs may appear:
- Cyanosis (bluish skin, especially with other defects)
- Fatigue and exercise intolerance
- Heart murmur (detected during routine exam)
- Arrhythmias (irregular heartbeats)
- Signs of heart failure (poor feeding, rapid breathing, sweating)
Diagnosis
- Fetal echocardiography can detect the condition before birth (though it is often missed).
- Postnatal echocardiogram confirms the anatomy.
- Electrocardiogram (ECG) and chest X‑ray help assess heart function and size.
Treatment Options
There is no cure, but surgical interventions can reroute blood flow more efficiently:
| Procedure | Goal |
|---|---|
| Double Switch Operation | Restores the left ventricle to systemic circulation (most complex, performed at specialized centers like Michigan Medicine). |
| Pacemaker Implantation | Treats associated heart block (a common complication). |
| Medication | Manages heart failure symptoms (diuretics, ACE inhibitors). |
| Heart Transplantation | Considered when the right ventricle fails despite all other measures. |
The double switch operation is the gold standard for suitable candidates. It requires a surgical team that performs such procedures regularly – hence the monopoly of a few high‑volume centers like Mott Children’s Hospital.
FAQ
Q: Is CCTGA always life‑threatening?
A: Not immediately. Some patients with isolated CCTGA (no other defects) live into adulthood without symptoms. However, the right ventricle is not designed for lifelong systemic work, so most will eventually develop heart failure, often in their 30s or 40s.
Q: Why couldn’t Jibran go to another hospital?
A: The double switch operation is extremely technically demanding. Only a handful of U.S. centers perform it routinely. Michigan Medicine’s Mott Children’s Hospital is the only such center in the state. Traveling out‑of‑state would add immense financial and logistical stress to the family.
Q: Did the contract dispute affect Jibran’s immediate care?
A: While he continued receiving care during the negotiations, the uncertainty threatened his long‑term follow‑up and any future surgeries. The resolution removes that threat.
Q: What can families do if they face a similar insurance‑hospital dispute?
A: Contact your state’s insurance commissioner, seek media attention (as Jibran’s family did), and ask for a “continuity of care” exception. Also, inquire about financial assistance programs at the hospital.
Q: Can CCTGA be detected before birth?
A: Yes, with a detailed fetal echocardiogram. However, subtle forms are sometimes missed. Routine prenatal ultrasounds may not catch it unless the sonographer specifically looks for ventricular morphology.
CCTGA, congenital heart defect, Blue Cross Michigan Medicine agreement, rare heart condition, double switch operation, congenitally corrected transposition of the great arteries, Michigan Medicine heart surgery, BCBSM contract dispute 2026 , CCTGA