The Origin
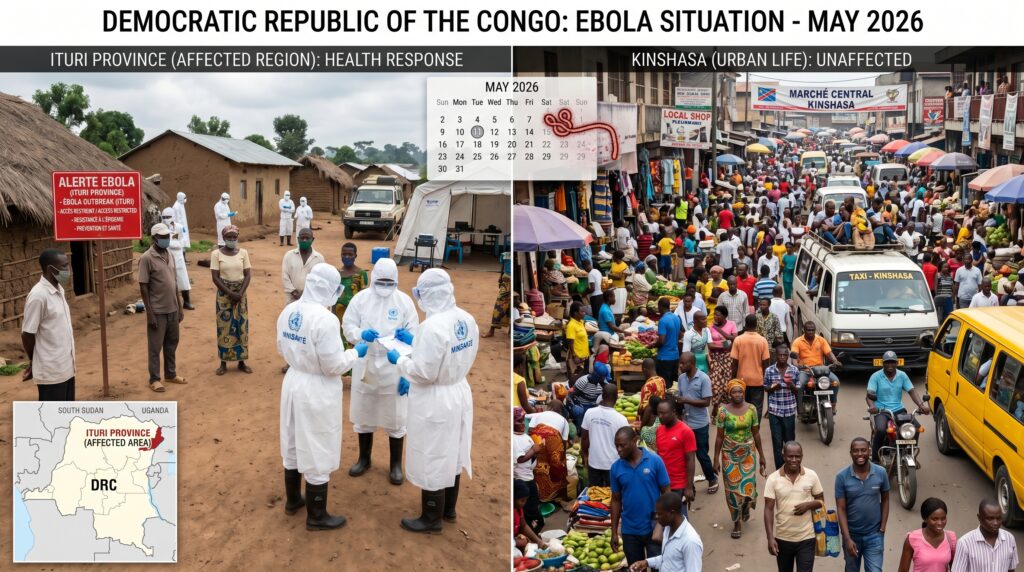
The outbreak began in late April 2026 in the rural Ituri Province of northeastern DRC. It was officially confirmed by health authorities in mid-May.
The Strain
Authorities identified the pathogen as the Bundibugyo ebolavirus. This is a major concern because, unlike the more common Zaire strain of Ebola, there are currently no approved vaccines or targeted therapeutics available for the Bundibugyo strain.
Rapid Spread
The virus has spread rapidly due to the region’s insecurity, a high volume of mining-related travel, and a local humanitarian crisis. By late May, hundreds of suspected cases and over a hundred deaths were reported. The virus successfully crossed borders, with confirmed cases in Kampala, Uganda, and has also reached the DRC’s capital, Kinshasa.
External Link: The World Health Organization (WHO) maintains an updated situation report on the outbreak. Read more here.
The Global and Local Response
International Emergency
On May 17, 2026, the World Health Organization (WHO) declared the outbreak a Public Health Emergency of International Concern (PHEIC) .
Travel Restrictions
In response to the outbreak’s spread, the United States recently instituted travel restrictions, requiring citizens and permanent residents departing from affected countries to fly into designated U.S. airports for screening. This move has drawn criticism from some Congo health officials.
External Link: The CDC provides updated travel guidance for the DRC and neighboring countries. Check here .
The Situation in Kinshasa
The headline you shared reflects the immense challenge of infectious disease control. Despite cases being identified in Kinshasa, residents continue to pack into markets, bars, and public transit. Imposing strict quarantines or social distancing in dense, highly informal urban economies is notoriously difficult, as a vast majority of the population relies on daily public interaction to survive.
Public health officials and the WHO are currently racing to deploy experimental vaccines and treatments, emphasizing grassroots community engagement to fight misinformation and encourage safe sanitation and burial practices.
Key Facts Summary
| Element | Detail |
|---|---|
| Virus Strain | Bundibugyo ebolavirus |
| Start Date | Late April 2026 |
| Epicenter | Ituri Province, northeastern DRC |
| Spread To | Kampala (Uganda), Kinshasa (DRC capital) |
| WHO Declaration | PHEIC – May 17, 2026 |
| Vaccine Available? | No (no approved vaccine for Bundibugyo strain) |
| U.S. Travel Restrictions | Yes – screening at designated airports |
What Makes the Bundibugyo Strain Different?
Most people are familiar with the Zaire ebolavirus (the strain responsible for the 2014-2016 West Africa epidemic), for which there is an effective vaccine (Ervebo). The Bundibugyo strain has several distinct characteristics:
- Lower mortality rate historically (30-50% vs. 50-90% for Zaire)
- No approved vaccine – existing vaccines do not protect against Bundibugyo
- Human-to-human transmission documented – similar to Andes hantavirus, this strain can spread through close contact with bodily fluids
- Longer incubation period (up to 21 days, similar to other Ebola strains)
This combination of factors—no vaccine, human transmission, and spread to a major urban center—is why the WHO declared a PHEIC.
FAQ
Q: Should travelers be concerned about visiting Kinshasa right now?
A: The CDC and WHO have issued travel advisories for the DRC. Non-essential travel to affected provinces is discouraged. Travelers should monitor official sources and practice strict hygiene.
Q: Can the Bundibugyo strain be treated?
A: There is no specific antiviral treatment. Supportive care (IV fluids, electrolyte management, oxygen) improves survival. Experimental therapeutics are being deployed in the DRC under compassionate use protocols.
Q: Is there a risk of this outbreak becoming a global pandemic?
A: WHO officials have stated that while the PHEIC declaration raises the alarm, Ebola does not spread through the air like COVID-19. With aggressive contact tracing and community cooperation, the outbreak can be contained regionally.
Q: Why is Kinshasa not in lockdown despite confirmed cases?
A: Kinshasa’s economy is largely informal; daily wages depend on market activity. A strict lockdown would cause widespread hunger and civil unrest. Health officials are focusing on targeted isolation, safe burials, and public awareness campaigns rather than city-wide shutdowns.
Ebola outbreak 2026
Bundibugyo strain
Kinshasa Ebola
WHO PHEIC May 2026
DRC travel restrictions
africa