If you have spent years battling chronic, unexplained bloating, you may have been told you simply have Irritable Bowel Syndrome (IBS) or that you just need to manage your stress. However, a significant portion of these cases are driven by an underlying—and treatable—condition: Small Intestinal Bacterial Overgrowth (SIBO) .
Research suggests that anywhere from 30% to 78% of patients diagnosed with IBS actually have SIBO. Because it requires specialized testing to identify, it remains one of the most frequently missed causes of chronic digestive distress.
Let me introduce you to Jennifer, a 42‑year‑old graphic designer who had been told she had IBS for over a decade. “I lived on antacids and avoided social events because the bloating was so embarrassing,” she told me. “Every doctor said the same thing: ‘It’s just IBS. Manage your stress.'”
Jennifer’s symptoms didn’t improve with stress management. After pushing for specialized testing, she finally received a diagnosis of SIBO. A course of targeted treatment, combined with dietary changes and addressing her underlying low stomach acid, completely transformed her digestion. “I spent ten years believing this was just how my body was,” she says. “I didn’t know it was fixable.”
Jennifer’s story is not uncommon. Here is what you need to know.
External Link: A 2020 meta‑analysis found that SIBO prevalence in IBS patients ranges from 30% to 78%. Read more here.
What Is SIBO?
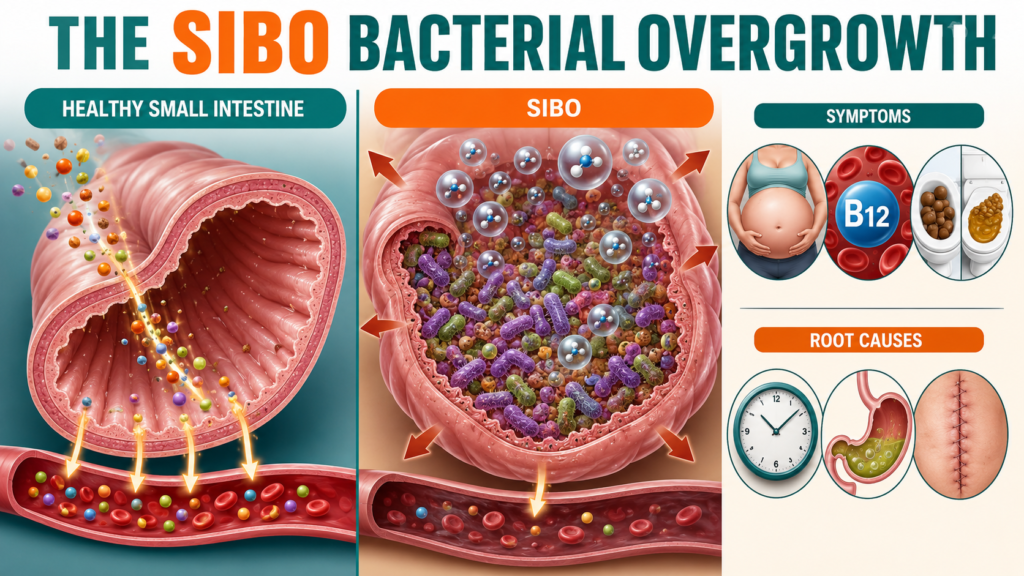
Your large intestine is naturally home to trillions of essential bacteria that make up your microbiome. Your small intestine, however, is designed to be relatively sterile so it can focus on absorbing nutrients from your food.
SIBO occurs when bacteria from the large intestine migrate upward—or when the small amount of native bacteria over‑multiplies—in the small intestine.
When these misplaced bacteria encounter food (especially carbohydrates and sugars) in your small intestine, they prematurely ferment it. This premature fermentation creates a massive release of hydrogen or methane gas, which stretches the intestinal walls and triggers intense discomfort.
Internal Link: SIBO is closely related to gut dysbiosis. Read The Dysbiosis Blueprint: The Silent Gut Collapse Sabotaging Your Metabolism.
The Core Symptoms of SIBO
SIBO symptoms can range from mild to debilitating, and they often worsen progressively throughout the day as you eat more meals.
| Symptom | How It Manifests |
|---|---|
| Severe Bloating | The abdomen visibly distends; many describe feeling “six months pregnant” by the evening |
| Bowel Changes | Chronic diarrhea (hydrogen gas) or persistent constipation (methane gas) |
| Excess Gas | Uncomfortable trapped wind, frequent belching, and flatulence |
| Fatigue & Deficiencies | Bacteria consume food before absorption; leads to low iron, B12 deficiency, and chronic exhaustion |
| Food Reactions | Healthy, fiber‑rich foods (garlic, onions, apples) suddenly trigger severe digestive distress |
Why Doctors Frequently Miss It
SIBO is often overlooked in standard medical practices for three key reasons:
1. The IBS Overlap
Because the symptoms perfectly mimic IBS, many doctors stop investigating once an IBS diagnosis is handed down. IBS is often treated as a final diagnosis rather than a symptom of a deeper issue. However, research shows that IBS is frequently a clinical presentation of underlying SIBO.
2. Standard Tests Don’t Catch It
Routine blood panels, stool tests, colonoscopies, and endoscopies look for inflammation, ulcers, or structural damage. They do not measure bacterial gas levels in the small intestine. SIBO is invisible to most standard gastrointestinal workups.
3. Lack of Awareness
While awareness is growing, many general practitioners are not trained in the nuances of functional gut dysbiosis. Most medical schools do not include SIBO in their core gastroenterology curriculum, leaving clinicians unprepared to identify or treat it.
The Diagnostic Solution: The Breath Test
To accurately diagnose SIBO, doctors must order a specific, non‑invasive hydrogen and methane breath test. This test measures the exact gases produced by the bacteria after you drink a specialized sugar solution. Fasting and dietary preparation are required before the test to ensure accurate results.
Internal Link: Leaky gut and SIBO often co‑exist. Read Leaky Gut Syndrome 2026: Science‑Backed Realities.
The Root Causes: Why Does SIBO Happen?
SIBO does not happen out of nowhere. It is almost always a secondary condition caused by a breakdown in the gut’s natural defense mechanisms.
1. Slowed Gut Motility
Between meals, your digestive tract generates “cleaning waves” that sweep leftover food and bacteria downward. If this movement slows due to nerve damage from a past bout of food poisoning, chronic stress, or hypothyroidism, bacteria are not cleared out properly.
2. Low Stomach Acid
Stomach acid acts as a harsh gatekeeper, killing off ingested bacteria before they reach the small intestine. Prolonged use of acid‑reducing medications (like PPIs) weakens this defense.
3. Structural Issues
Adhesions or scar tissue from prior abdominal surgeries (such as C‑sections, appendectomies, or endometriosis excisions) can create physical roadblocks where bacteria pool and multiply.
4. Other Contributing Factors
| Factor | Mechanism |
|---|---|
| Food Poisoning | Damages the migrating motor complex (MMC), reducing gut motility |
| Antibiotic Use | Disrupts the microbiome, allowing opportunistic bacteria to overgrow |
| Chronic Stress | Suppresses stomach acid and reduces blood flow to the gut |
| Hypothyroidism | Slows down the entire digestive tract |
The SIBO Treatment Framework
Properly treating SIBO requires more than just clearing the bacteria with targeted antibiotics (like Rifaximin) or herbal antimicrobials; it requires identifying and fixing the underlying root cause so the overgrowth does not simply return a few months later.
Phase 1: Clear the Overgrowth
- Antibiotics: Rifaximin (for hydrogen‑dominant SIBO) or Rifaximin + Neomycin (for methane‑dominant SIBO).
- Herbal Antimicrobials: Alternative for those who prefer natural options (e.g., Allicin, Berberine, Oregano Oil) – though they may be less potent than Rifaximin.
Phase 2: Restore Motility
- Prokinetics: Medications or supplements (like ginger and artichoke extract) that stimulate the migrating motor complex (MMC) to prevent recurrence.
Phase 3: Address the Root Cause
- Treat hypothyroidism if present.
- Taper off PPIs if they are no longer medically necessary.
- Manage stress to support vagal tone and gut motility.
Phase 4: Repair the Gut
- Support the intestinal lining with L‑Glutamine, zinc carnosine, and collagen peptides.
- Rebuild the microbiome with targeted probiotics (once the SIBO is cleared).
Internal Link: Gut repair is a foundational step. Read The Gut Reset Protocol: Repairing Your Intestinal Barrier for Metabolic Resilience.
The SIBO vs. IBS Matrix
| Feature | IBS | SIBO |
|---|---|---|
| Underlying Cause | Unclear; often a diagnosis of exclusion | Bacterial overgrowth in the small intestine |
| Diagnosis | Based on symptom criteria (Rome IV) | Confirmed via hydrogen/methane breath test |
| Prevalence in IBS Patients | 100% | 30‑78% |
| Treatment | Symptom management (diet, stress, medications) | Targeted antimicrobials + root cause resolution |
| Can It Be Cured? | Managed, not always cured | Often cured when root cause is resolved |
The Bottom Line: Stop Accepting IBS as the Final Answer
Jennifer now follows a maintenance protocol: a prokinetic at night, regular stress management, and a diet that supports her gut motility. “I stopped accepting that my body was broken,” she says. “I got tested, got treated, and got my life back.”
If you have been diagnosed with IBS and still struggle with chronic bloating, digestive distress, or unexplained fatigue, do not accept IBS as the final answer. Ask your doctor about a hydrogen and methane breath test for SIBO.
FAQ: SIBO
Q: What is the difference between SIBO and IBS?
A: IBS is a functional disorder diagnosed based on symptom criteria (Rome IV). SIBO is a specific, measurable condition where bacteria overgrow in the small intestine. Research shows that 30‑78% of IBS patients actually have SIBO as the underlying cause of their symptoms.
Q: How do you test for SIBO?
A: The gold standard is the hydrogen and methane breath test. You drink a specialized sugar solution (lactulose or glucose), and your breath is sampled every 15‑20 minutes for 2‑3 hours. The test measures the gases produced by bacteria fermenting the sugar in your small intestine.
Q: Is SIBO curable?
A: Yes, in many cases. However, it requires identifying and treating the root cause. If the underlying motility issue, low stomach acid, or structural problem is not addressed, SIBO is likely to recur.
Q: What foods trigger SIBO symptoms?
A: High‑FODMAP foods (fermentable carbohydrates) are the most common triggers: garlic, onions, wheat, beans, apples, and dairy. These are fermented rapidly by the bacteria, causing gas production and bloating.
Q: Can SIBO cause nutrient deficiencies?
A: Yes. The bacteria in the small intestine consume nutrients before your body can absorb them. Common deficiencies include vitamin B12, iron, vitamin D, and fat‑soluble vitamins (A, D, E, K) .
Q: Do probiotics help or worsen SIBO?
A: It depends on the strain and timing. Some probiotics can help restore gut health after SIBO is cleared. However, certain strains may contribute to bacterial overgrowth during active infection. Always work with a practitioner knowledgeable in SIBO before using probiotics.
Q: Can SIBO cause weight gain or weight loss?
A: Both are possible. Methane‑dominant SIBO is often associated with constipation and weight gain (as methane slows motility). Hydrogen‑dominant SIBO is often associated with diarrhea and weight loss (as malabsorption occurs).
SIBO
small intestinal bacterial overgrowth
SIBO symptoms
SIBO test
SIBO vs IBS
SIBO treatment
hydrogen methane breath test
IBS SIBO overlap
SIBO root causes
sibo breath test
test for sibo
sibo reddit
small intestinal bacterial overgrowth